
Subscribe to RSS
DOI: 10.1055/a-2646-7702
Are Intravenous Subnarcotic Ketamine Infusions as an Adjunct Treatment for Treatment-Resistant Depression Ready to be Recommended in European Guidelines?

Dear Editor
Esketamine nasal spray (EN; Spravato) has been gaining traction in the national treatment guidelines of Western countries for use as an augmentation strategy in treatment-resistant unipolar depression (TRD) since its approval by the FDA and EMA in 2019 (e. g., [1]). EN’s treatment approach for TRD has been historically informed by the increasing number of observational studies and subsequent randomized clinical trials (beginning in 2000) demonstrating that add-on subnarcotic intravenous ketamine (SIK) can offer temporary relief for TRD [2]. However, SIK has not received approval from any regulatory authority for the treatment of TRD, and it is improbable that this will occur in the future due to a lack of patent protection for this application (resulting in no interest from the pharmaceutical industry to carry out prospective randomized two-arm (SIK vs. EN) or even three-arm studies (placebo vs. SIK vs. EN)).
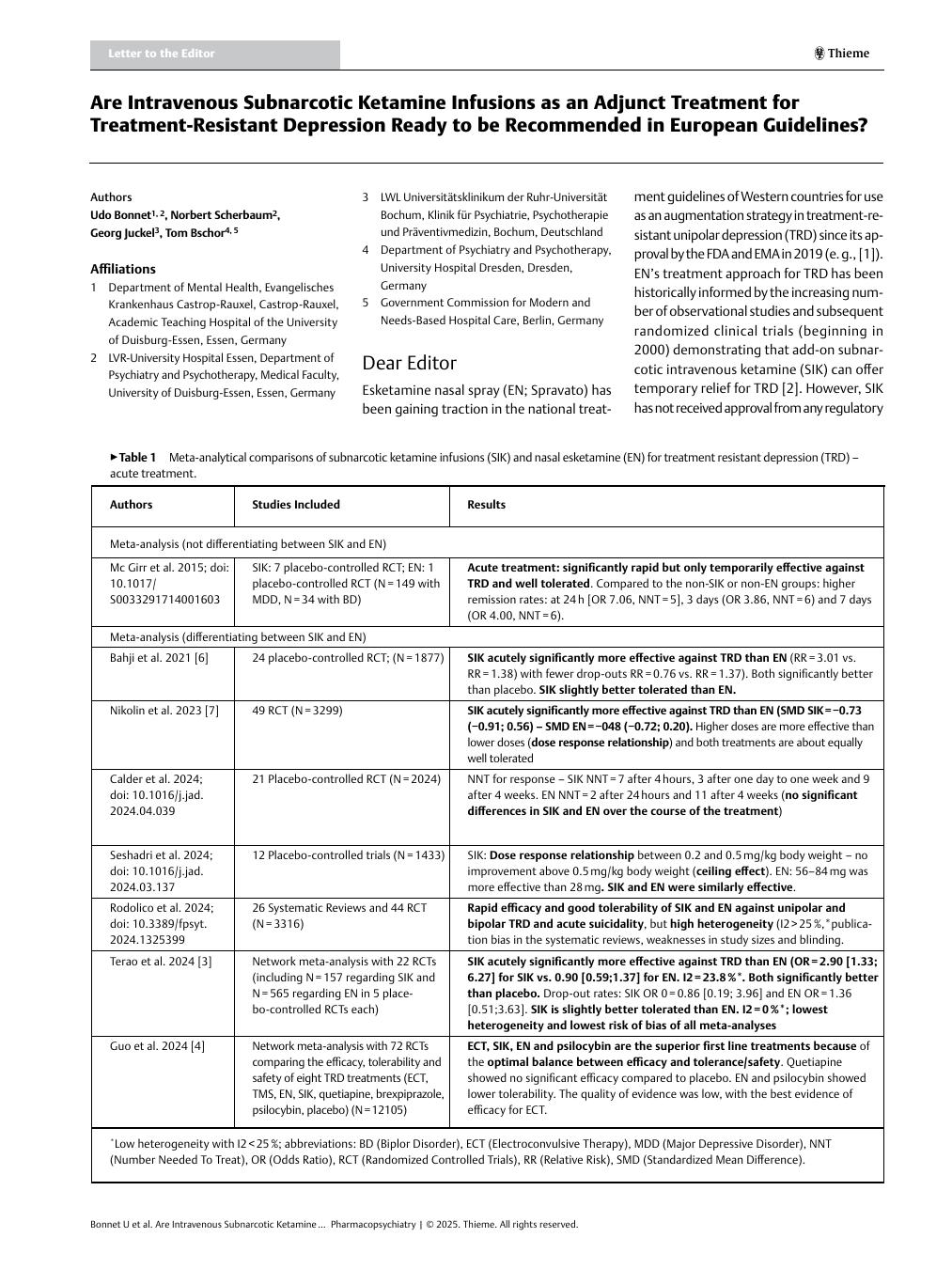
Over the past year, two valid network meta-analyses [3] [4] and several retrospective comparative observational studies [5] have demonstrated that off-label SIK is at least equally successful, tolerable, and safe as in-label EN when used as an add-on treatment for TRD. Before this, there were multiple meta-analyses, most of which indicated this result ([Table 1]). Remarkably, the direct costs for SIK are about 1000 times lower. Furthermore, SIK demonstrated a superior response compared to EN in a couple of studies [3] [5] [6] [7].
|
Authors |
Studies Included |
Results |
|---|---|---|
|
Meta-analysis (not differentiating between SIK and EN) |
||
|
Mc Girr et al. 2015; doi:10.1017/S0033291714001603 |
SIK: 7 placebo-controlled RCT; EN: 1 placebo-controlled RCT (N=149 with MDD, N=34 with BD) |
Acute treatment: significantly rapid but only temporarily effective against TRD and well tolerated. Compared to the non-SIK or non-EN groups: higher remission rates: at 24 h [OR 7.06, NNT=5], 3 days (OR 3.86, NNT=6) and 7 days (OR 4.00, NNT=6). |
|
Meta-analysis (differentiating between SIK and EN) |
||
|
Bahji et al. 2021 [6] |
24 placebo-controlled RCT; (N=1877) |
SIK acutely significantly more effective against TRD than EN (RR=3.01 vs. RR=1.38) with fewer drop-outs RR=0.76 vs. RR=1.37). Both significantly better than placebo. SIK slightly better tolerated than EN. |
|
Nikolin et al. 2023 [7] |
49 RCT (N=3299) |
SIK acutely significantly more effective against TRD than EN (SMD SIK=−0.73 (−0.91; 0.56) – SMD EN=−048 (−0.72; 0.20). Higher doses are more effective than lower doses (dose response relationship) and both treatments are about equally well tolerated |
|
Calder et al. 2024; doi:10.1016/j.jad.2024.04.039 |
21 Placebo-controlled RCT (N=2024) |
NNT for response – SIK NNT=7 after 4 hours, 3 after one day to one week and 9 after 4 weeks. EN NNT=2 after 24 hours and 11 after 4 weeks (no significant differences in SIK and EN over the course of the treatment) |
|
Seshadri et al. 2024; doi: 10.1016/j.jad.2024.03.137 |
12 Placebo-controlled trials (N=1433) |
SIK: Dose response relationship between 0.2 and 0.5 mg/kg body weight – no improvement above 0.5 mg/kg body weight (ceiling effect). EN: 56–84 mg was more effective than 28 mg. SIK and EN were similarly effective. |
|
Rodolico et al. 2024; doi: 10.3389/fpsyt.2024.1325399 |
26 Systematic Reviews and 44 RCT (N=3316) |
Rapid efficacy and good tolerability of SIK and EN against unipolar and bipolar TRD and acute suicidality, but high heterogeneity (I2>25%,*publication bias in the systematic reviews, weaknesses in study sizes and blinding. |
|
Terao et al. 2024 [3] |
Network meta-analysis with 22 RCTs (including N=157 regarding SIK and N=565 regarding EN in 5 placebo-controlled RCTs each) |
SIK acutely significantly more effective against TRD than EN (OR=2.90 [1.33; 6.27] for SIK vs. 0.90 [0.59;1.37] for EN. I2=23.8%*. Both significantly better than placebo. Drop-out rates: SIK OR 0=0.86 [0.19; 3.96] and EN OR=1.36 [0.51;3.63]. SIK is slightly better tolerated than EN. I2=0%*; lowest heterogeneity and lowest risk of bias of all meta-analyses |
|
Guo et al. 2024 [4] |
Network meta-analysis with 72 RCTs comparing the efficacy, tolerability and safety of eight TRD treatments (ECT, TMS, EN, SIK, quetiapine, brexpiprazole, psilocybin, placebo) (N=12105) |
ECT, SIK, EN and psilocybin are the superior first line treatments because of the optimal balance between efficacy and tolerance/safety. Quetiapine showed no significant efficacy compared to placebo. EN and psilocybin showed lower tolerability. The quality of evidence was low, with the best evidence of efficacy for ECT. |
*Low heterogeneity with I2<25%; abbreviations: BD (Biplor Disorder), ECT (Electroconvulsive Therapy), MDD (Major Depressive Disorder), NNT (Number Needed To Treat), OR (Odds Ratio), RCT (Randomized Controlled Trials), RR (Relative Risk), SMD (Standardized Mean Difference).
We believe that the encouraging results for SIK should be taken into account in future European guidelines regarding MDD treatment. Is the off-label status of SIK adequate to endorse this treatment option as clearly secondary to EN in the acute management of TRD? We think that if the necessary informed consent and documentation requirements for off-label prescriptions are fulfilled, the answer should be no.
We believe that in countries where health insurance reimbursement is contingent on a medication’s approval status, health insurance companies should not have any insurmountable objections, given the lower treatment costs and relatively favorable risk:benefit profile of SIK. If there is uncertainty, they could be requested to pay for the treatment prior to the initiation of off-label SIK treatment.
A recent statement by the National Network of Depression Centers in the USA supports insurance coverage for SIK in cases of TRD [5]. To our knowledge, Europe still lacks such statements, and this letter aims to promote their development and provides a first advance. In its guidelines for treating TRD, the French Society for Biological Psychiatry and Neuropsychopharmacology has recently advised using EN as a first-line add-on agent and SIK as a second-line add-on agent, though the latter is off-label [8].
Lastly, it is also worth noting that the USA [9] and Canada [10] have already incorporated off-label SIK as an alternative to approved EN in their MDD treatment guidelines. However, data on maintenance therapy with SIK is even more limited than for EN. Nevertheless, initial meta-analyses do suggest results that could justify a recommendation in this area too ([Table 2]).
|
Authors |
Studies Included |
Results |
|---|---|---|
|
Marcantoni et al. 2020; 10.1016/j.jad.2020.09.007 |
SIK: 28 RCT (N=1000), Treatment duration: up to 12 weeks |
Multiple infusions increased and prolonged efficacy with good tolerability, I2>25%* |
|
Scott et al. 2023; doi: 10.1177/02698811221104058 |
115 RCTs (48 different types of augmentation) – including 4 RCTs each with EN and SIK (N=NA); mean treatment duration: 9 weeks |
SIK and EN together: ES=1.48 (1.23; 1.73), I2*>25%, high risk of bias |
|
Nunez et al. 2023; doi: 10.3390/brainSKI13121672 |
7 clinical trials with BD, including 2 RCT (N=33) and 5 non-randomized (N=159) – N=for SIK; N=140 for EN |
Response (54% vs. 55%) and remission rates (30% vs. 40%) for single and serial SIKs were similar. I2>25%*, high risk of bias. Data quality for EN was too poor |
*Low heterogeneity with I2<25%; abbreviations: BD (Biplolar Disorder), ES (Effect Size), RCT (Randomized Controlled Trials).
Letters to the editor do not necessarily represent the opinion of the editor or publisher. The editor and publisher reserve the right to not publish letters to the editor, or to publish them abbreviated or in extract.
Publication History
Received: 03 May 2025
Accepted: 30 June 2025
Article published online:
06 August 2025
© 2025. Thieme. All rights reserved.
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 NVL – Nationale Versorgungs-Leitlinie Unipolare Depression, 2022. Version 3.2, Juli 2023 https://www.leitlinien.de/themen/depression/version-3 (Accessed date May, 2th, 2025) [Guideline in German]
- 2 Johnston JN, Kadriu B, Kraus C. et al. Ketamine in neuropsychiatric disorders: an update. Neuropsychopharmacology 2024; 49: 23-40
- 3 Terao I, Tsuge T, Endo K. et al. Comparative efficacy, tolerability and acceptability of intravenous racemic ketamine with intranasal esketamine, aripiprazole and lithium as augmentative treatments for treatment-resistant unipolar depression: A systematic review and network meta-analysis. J Affect Disord 2024; 346: 49-56
- 4 Guo Q, Guo L, Wang Y. et al. Efficacy and safety of eight enhanced therapies for treatment-resistant depression: A systematic review and network meta-analysis of RCTs. Psychiatry Res 2024; 339: 116018
- 5 Singh B, Kung S, Vande Voort JL. Intravenous (IV) ketamine versus intranasal esketamine for depression – Advantage IV ketamine?. J Affect Disord 2024; 356: 564-567
- 6 Bahji A, Vazquez GH, Zarate CA. Comparative efficacy of racemic ketamine and esketamine for depression: A systematic review and meta-analysis. J Affect Disord 2021; 278: 542-555
- 7 Nikolin S, Rodgers A, Schwaab A. et al. Ketamine for the treatment of major depression: a systematic review and meta-analysis. EClinicalMedicine 2023; 62: 102127
- 8 Yrondi A, Javelot H, Nobile B. et al. French Society for Biological Psychiatry and Neuropsychopharmacology (AFPBN) guidelines for the management of patients with partially responsive depression and treatment-resistant depression: Update 2024. Encephale 2025; 51: 26-38
- 9 VA/DoD Clinical Practice Guideline. The Management of Major Depressive Disorder. Washington 2022, DC: U.S. Government Peinting Office https://www.healthquality.va.gov/guidelines/MH/mdd/VADODMDDCPGFinal508.pdf (Accessed date May, 2th, 2025)
- 10 Lam RW, Kennedy SH, Adams C. et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults: Réseau canadien pour les traitements de l'humeur et de l'anxiété (CANMAT) 2023 : Mise à jour des lignes directrices cliniques pour la prise en charge du trouble dépressif majeur chez les adultes. Can J Psychiatry 2024; 69: 641-687